
The Convergence of AI and Precision Oncology

The landscape of oncology drug development in February 2026 is defined by a paradigm shift from broad-spectrum cytotoxic interventions to highly personalized, molecularly targeted therapies. This evolution has been significantly accelerated by the integration of artificial intelligence (AI) and machine learning (ML), which have moved beyond the initial stage of industry "hype" into a period of robust real-world evidence (RWE). As the pharmaceutical industry grapples with increasing complexity and rising research and development costs, the convergence of computational biology and precision oncology offers a measurable reduction in timelines, particularly during the critical transition from discovery to Phase I clinical trials.
The fiscal year 2026 budget for the National Institutes of Health (NIH) underscores this commitment to innovation, with a total allocation of $47.2 billion, including a dedicated $7.35 billion for the National Cancer Institute (NCI). These investments, combined with a historic transatlantic regulatory alignment between the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) in January 2026, provide a standardized framework for the deployment of AI in drug development. This report examines the empirical impact of AI-driven drug discovery on Phase I oncology timelines and the resulting shifts in market entry strategies for global biopharmaceutical stakeholders.
The Macro-Economic and Funding Landscape in 2026
The financial foundation for precision oncology has reached a state of stabilization in early 2026 following a period of budget uncertainty in 2025. The enactment of the fiscal year 2026 spending package on February 3, 2026, provided a modest but critical increase for federal medical research. This funding is essential for the basic mechanistic research into biological and genetic causes of cancer disparities, which increasingly utilizes new computational approaches to discover and test biological mechanisms.
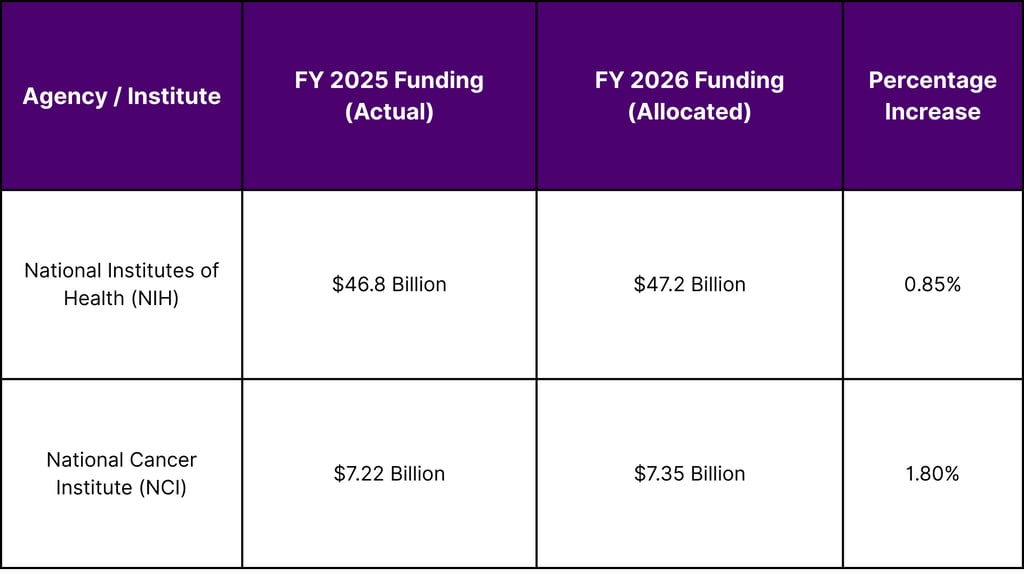

The increase in NCI funding is particularly significant for the development of new 3D cellular models, organoids, and patient-derived models designed to recapitulate cancer health disparities. These models provide the high-quality data necessary for training AI algorithms that can predict therapeutic responses across diverse patient populations.
Technological Transformation of the Oncology Discovery Pipeline
Traditionally, the path from target identification to the initiation of Phase I clinical trials has been an arduous process spanning four to seven years. The integration of AI has fundamentally altered this timeline by enhancing productivity in drug discovery and preclinical testing. By leveraging machine learning (ML), deep learning (DL), and natural language processing (NLP), researchers can now integrate massive, multimodal datasets, including genomic profiles and clinical outcomes, to identify druggable targets with greater precision.
Shortening the Path to Phase I
One of the most profound impacts of AI in 2026 is the compression of the early discovery phase. Traditional lead identification and optimization often require the synthesis and screening of thousands of compounds over three to six years. AI-integrated workflows have demonstrated the ability to reduce the number of compounds needing synthesis by up to 85%. For instance, predictive models can find a promising candidate after exploring only 350 compounds, compared to the 2,500 compounds typically required in conventional approaches.
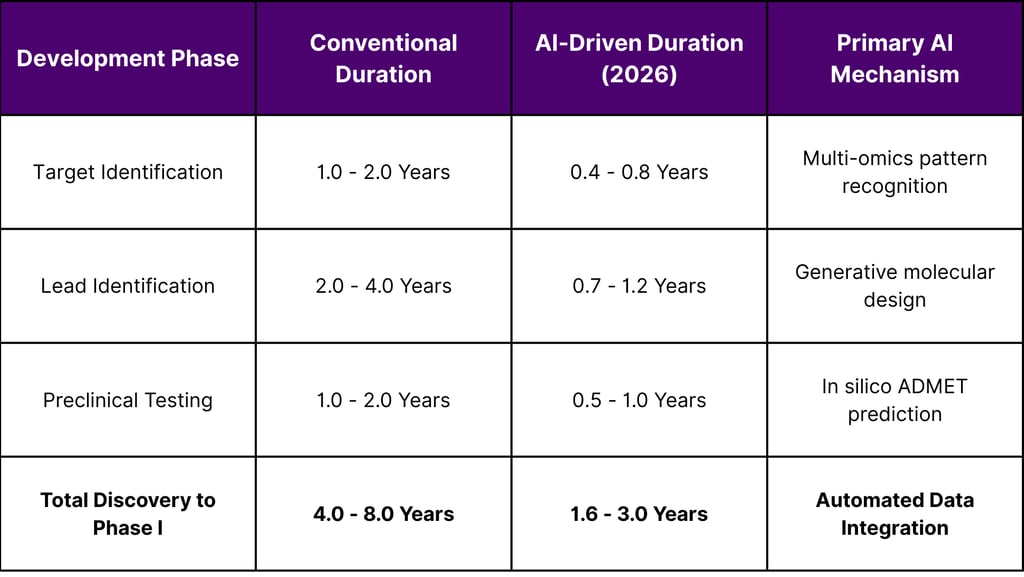

This compression allows AI-discovered drugs to reach the clinic in roughly 13 to 18 months, compared to the traditional average of four to five years. By February 2026, the industry has seen over 173 AI-designed programs enter clinical development, a significant increase from just 67 programs in 2023.
Advancements in ADMET and Predictive Toxicology
A major cause of attrition in early-stage drug development is inferior absorption, distribution, metabolism, excretion, and toxicity (ADMET) profiles. AI improves the success rates of molecules by performing early-stage assessments of these properties through automated data analysis and molecular modeling. By identifying potential toxicity or efficacy issues in silico, sponsors can drop problematic candidates sooner and prioritize those with higher probabilities of clinical success.
Phase I Clinical Success: Moving Beyond Hype
While the speed of discovery is a compelling metric, the true measure of AI’s impact is the clinical performance of the resulting molecules. In 2026, empirical evidence from the clinical pipelines of AI-native biotech companies has begun to silence skeptics.
Empirical Success Rates in 2026
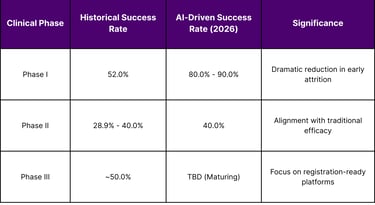
Historical data for oncology indicates that only about 10% of drugs that enter Phase I ultimately receive regulatory approval.1 However, an analysis of AI-discovered molecules in Phase I trials shows a success rate of 80% to 90%. This suggests that AI is highly capable of identifying molecules with superior "drug-like" properties and safety profiles.
The success rates in Phase II remain comparable to historical industry averages at approximately 40%, indicating that proving clinical efficacy in broader, more heterogeneous patient populations remains a significant biological challenge. Nevertheless, the cumulative probability of success from Phase I to approval is substantially improved when the initial candidates are selected through AI-enabled workflows.
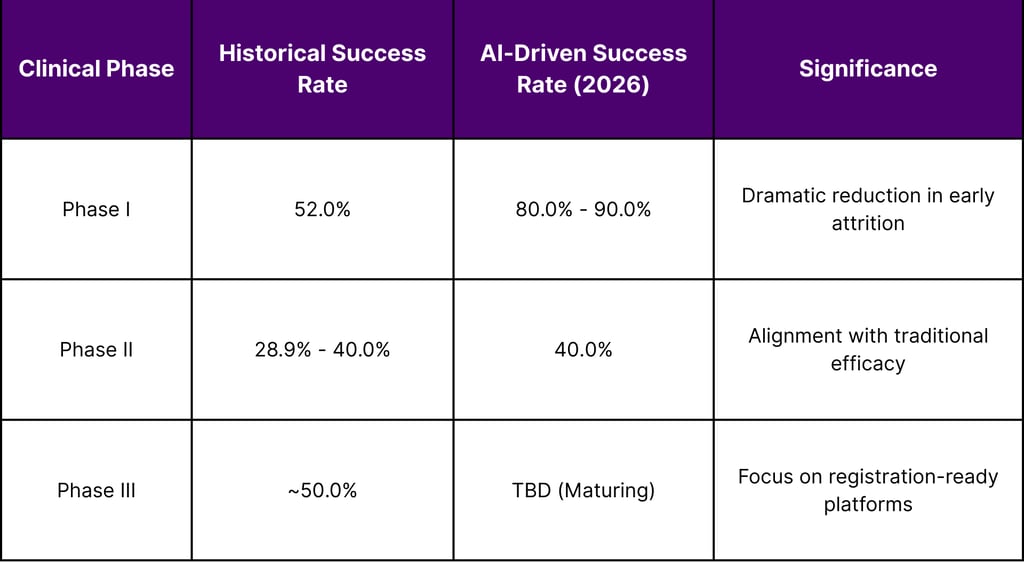
The high success rate in Phase I is attributed to AI's ability to predict off-target interactions and optimize dosing strategies before human exposure. Furthermore, AI-driven biomarkers are used to stratify patients more effectively, ensuring that Phase I trials enroll individuals most likely to tolerate the drug and show early signals of response.
Regulatory Evolution: The 2026 FDA and EMA Frameworks
The maturation of AI in oncology would not be possible without a corresponding evolution in regulatory oversight. In early 2026, the FDA and EMA have transitioned from exploratory discussions to the implementation of concrete, risk-based frameworks for AI-enabled drug development.
The Joint Guiding Principles (January 2026)
On January 14, 2026, the FDA and EMA published a landmark joint document titled "Guiding Principles of Good AI Practice in Drug Development". This transatlantic alignment provides ten core principles for how AI should be built, used, and monitored throughout the pharmaceutical lifecycle.
Human-centric by Design: AI technologies must align with ethical values and involve human oversight.
Risk-based Approach: Validation and oversight must be proportionate to the context of use (COU).
Adherence to Standards: Compliance with GxP, cybersecurity, and regulatory standards is mandatory.
Clear Context of Use: The role and scope of the AI technology must be well-defined.
Multidisciplinary Expertise: Integration of AI and clinical expertise is required across the lifecycle.
Data Governance: Processing steps and data provenance must be documented and verifiable.
Model Design: Development must focus on explainability, interpretability, and predictive performance.
Performance Assessment: Evaluation of the complete human-AI system using appropriate metrics.
Lifecycle Management: Implementation of risk-based quality management systems to address algorithm drift.
Transparency: Provision of clear, essential information to patients and users.
This alignment is critical for market entry strategies, as it ensures that data generated through AI-driven models in the United States will be more readily accepted by European regulators, and vice-versa.
FDA Oncology Center of Excellence (OCE) AI Program
The FDA’s OCE Oncology AI Program, established in 2023, has become the primary regulatory touchpoint for oncology sponsors. By February 2026, the program has focused on streamlining the review process for applications that incorporate AI technologies, offering specialized training for reviewers and supporting regulatory science research.
Recent guidance from the FDA includes a risk-based credibility assessment framework to evaluate the performance of AI models for a particular context of use. Additionally, the Predetermined Change Control Plan (PCCP) allows sponsors to update AI models to control algorithm drift without requiring new FDA approval for every iteration, a significant step in facilitating the clinical use of AI.
Precision Oncology and the New Biomarker Paradigm
AI is particularly powerful in identifying complex biomarker signatures that guide patient selection and predict responses to targeted therapies. In 2026, the integration of multi-omics data genomics, transcriptomics, proteomics, and metabolomics is the standard for uncovering hidden patterns that traditional statistical methods might miss.
Digital Twins and In Silico Screening
The concept of "digital twins" virtual patient models simulated through AI has moved from theory to pilot implementation in oncology trials. These models allow for the virtual testing of drugs before clinical trials begin, helping to select the most appropriate endpoints and stratify patients effectively. By simulating multiple scenarios, researchers can optimize trial designs and reduce the number of patients required, thereby accelerating enrollment and completion.
Case Study: Lantern Pharma’s RADR® Platform
Lantern Pharma utilized its RADR® AI platform to identify PTGR1 as a key predictive biomarker for its LP-184 program. This AI-driven strategy allowed the company to identify that over 87% of patients in its Phase 1a study exceeded the bioactivation threshold for the drug. The trial demonstrated a 54% disease control rate in heavily pre-treated patients, enabling Lantern to advance into multiple biomarker-guided Phase 1b/2 trials across triple-negative breast cancer (TNBC), glioblastoma multiforme (GBM), and non-small cell lung cancer (NSCLC).
Market Entry Strategies: The "Registration-Ready" Advantage
The shortening of Phase I timelines has profound implications for the commercial strategies of biopharmaceutical companies. In 2026, the focus has shifted toward building "registration-ready" platforms that align with the evolving regulatory landscape.
Structural Rotation Toward Registration-Ready Platforms
By February 2026, the global oncology clinical trials market is seeing a structural rotation favoring platforms that demonstrate pivotal-trial alignment as early as Phase I. Sponsors are leveraging AI not just for molecule design, but for real-time adaptive trial designs that allow for modifications in dosing, stratification, or drug combinations based on predictive modeling.
Economics of AI-Driven Entry
The economic benefits of AI are significant. Clinical trial costs can be reduced by up to 70%, translating to billions in savings across the industry. For smaller biotech firms, this reduction in capital requirement lowers the barrier to entry, while for larger pharmaceutical companies, it allows for a more diversified and robust pipeline.
Patent Life Preservation: By reducing the discovery-to-clinic timeline by 2-3 years, companies can preserve a larger portion of the drug's patent life for commercialization.
Reduced Attrition Costs: With Phase I success rates rising to 80-90%, the "sunk cost" of early-stage failures is significantly mitigated.
Fast Track Alignment: The FDA’s use of Fast Track designations for AI-driven molecules such as SIGX1094 for gastric cancer further expedites the path to market.
Real-World Evidence vs. Hype: Addressing the Challenges
Despite the advancements, the oncology community in 2026 remains vigilant against over-reliance on AI. The "hype" of full autonomy is being countered by a "human-in-the-loop" (HITL) strategy centered on retrieval-augmented generation (RAG) and auditable governance.
Algorithmic Bias and Data Quality
A persistent challenge is the underrepresentation of minority groups in AI training datasets, which can lead to algorithmic bias in treatment recommendations. Ethical deployment requires robust regulatory frameworks and bias-aware validation to ensure that AI-driven precision oncology does not exacerbate existing health disparities.
The Gap Between Academic and Community Settings
There is a widening gap between the use of AI in NCI-designated cancer centers and community cancer centers. Smaller centers often lack the resources for vendor reviews and the technical infrastructure required for AI implementation.15 Bridging this gap is essential for the broad adoption of AI-driven precision oncology.
Algorithm Drift and Clinical De-skilling
The FDA’s focus on PCCPs addresses the risk of algorithm drift, where a model's performance degrades as it encounters new data. Furthermore, some studies suggest a risk of "de-skilling" among clinicians who become overly reliant on AI-assisted diagnostics, highlighting the need for continuous training and professional development in the era of AI.
Future Outlook: Oncology in 2026 and Beyond
As 2026 progresses, the convergence of AI and precision oncology is expected to redefine the standards of care. The American Cancer Society (ACS) reports that cancer survival rates have hit a historic 70% in 2026, a milestone driven by better early detection and more effective, targeted therapies.
The next five years will likely see:
Sustainable Workforce: AI-driven automation of administrative tasks and clinical decision support to alleviate oncologist burnout.
Personalized Screening: AI models that integrate genetic and socioeconomic factors for tailored screening programs.
Microbiome-Powered Therapies: Pairing precision nutrition with oncology treatments, as research indicates gut bacteria significantly influence drug metabolism.
Adaptive Radiotherapy: AI-assisted dose modification based on real-time interval imaging for high-grade gliomas.
The industry's trajectory suggests that AI will become the norm rather than the exception in every stage of the oncology pipeline, from the earliest identification of a druggable target to post-market safety monitoring.
Frequently Asked Questions (FAQ)
Q1: How does AI actually shorten the Phase I timeline in oncology?
AI shortens the timeline by automating target identification and lead optimization. By integrating multi-omics datasets and using generative molecular design, AI can identify a viable candidate in 13-18 months, compared to the traditional 3-6 years. It also optimizes patient matching, which can reduce recruitment timelines by up to 40%.
Q2: What is the significance of the January 2026 FDA/EMA Joint Guiding Principles?
This is the first transatlantic regulatory alignment on AI in drug development. It provides ten guiding principles (e.g., human-centricity, risk-based validation, and transparent data governance) that allow sponsors to build AI models that meet the standards of both major regulatory bodies, simplifying global market entry.
Q3: Are AI-designed drugs safer than traditionally developed drugs?
While "safety" must always be proven in clinical trials, AI-discovered molecules are achieving 80-90% success rates in Phase I trials (which primarily assess safety). This suggests that AI is better at predicting and avoiding off-target toxicities during the in silico design phase.
Q4: How does AI impact the cost of oncology clinical trials?
AI can reduce clinical trial costs by up to 70%. These savings come from reduced attrition (fewer failures), smaller required sample sizes through better patient stratification, and the use of adaptive trial designs that respond to data in real-time.
Q5: What is a Predetermined Change Control Plan (PCCP)?
A PCCP is a regulatory framework shared by the FDA that allows sponsors to specify how an AI model will be updated and improved over time. This helps manage "algorithm drift" without requiring a new regulatory submission for every iteration of the model.
References
American Association for Cancer Research. (2026, February 10). Cancer Policy Monitor: February 10, 2026.
European Medicines Agency. (2026, January 14). Principles for AI in medicine development.
European Medicines Agency. (2026, January). Final programming document 2026-2028. EMA/10240/2026.
U.S. Food and Drug Administration. (2025, January). Considerations for the Use of Artificial Intelligence To Support Regulatory Decision-Making for Drug and Biological Products: Draft Guidance for Industry.
U.S. Food and Drug Administration. (2026, February 13). FDA Grand Rounds 2026.
National Institutes of Health. (2025, November 27). A New Era of Artificial Intelligence (AI): Transforming Drug Discovery and Development. PMC12908618.
National Institutes of Health. (2026, February). Generative AI-based Interpretation of Genetic Mutations in Precision Oncology. PMC12896320.
Navigation
© 2026 FyreIgnis Market Research. All rights reserved.
Legal
info@fyreignismarketresearch.com
India
