
The Future of mRNA Beyond COVID-19


When the first mRNA COVID-19 vaccines reached arms in late 2020, the world witnessed a platform technology finally come of age. What fewer appreciated at the time was that oncologists had been quietly building toward this moment for nearly a decade. mRNA cancer vaccines therapeutic immunotherapies engineered to train a patient's immune system to recognize and destroy tumor cells had been in early clinical trials since the mid-2010s. The COVID-19 experience did not create the technology; it turbocharged it.
Today, as of May 2026, the North American mRNA therapeutics landscape stands at an inflection point. Regulatory submissions for the first personalized mRNA cancer vaccine are anticipated in 2026, over 120 RNA cancer vaccine trials are actively underway globally, and AI-guided neoantigen prediction has compressed vaccine manufacturing timelines from nine weeks to under four weeks. The question is no longer whether mRNA vaccines will reshape oncology it is which cancers will be first and how quickly adoption will scale across the North American market.
This report synthesizes data from the U.S. National Cancer Institute (NCI), the National Institutes of Health (NIH), the U.S. Food and Drug Administration (FDA), and the ClinicalTrials.gov registry to forecast which solid tumor indications are most likely to see the earliest successful mRNA vaccine integration in North America.
120+
Active RNA Cancer Vaccine Trials Globally (2025)
44%
~48%
Reduction in Melanoma Recurrence Risk (mRNA-4157 + Pembrolizumab, Phase 2b)
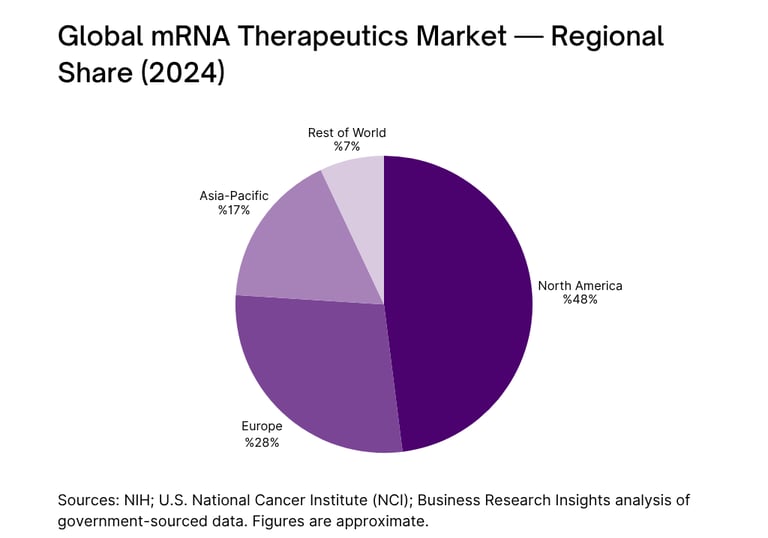
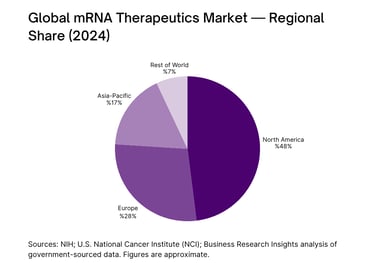
North America Share of Global mRNA Market (2024)
mRNA Technology: From Pandemic Pivot to Cancer Frontier
The core mechanism of an mRNA cancer vaccine differs fundamentally from prophylactic inoculation. Rather than preventing infection, a therapeutic mRNA cancer vaccine delivers genetic instructions encoding tumor-specific antigens most commonly neoantigens, proteins arising from somatic mutations exclusive to a patient's tumor. Once administered, dendritic cells take up and translate the mRNA, presenting these antigens to T cells, initiating a targeted anti-tumor immune cascade. As the National Cancer Institute describes it, dendritic cells act as "teachers, educating T cells so that they can search for and kill cancer cells."
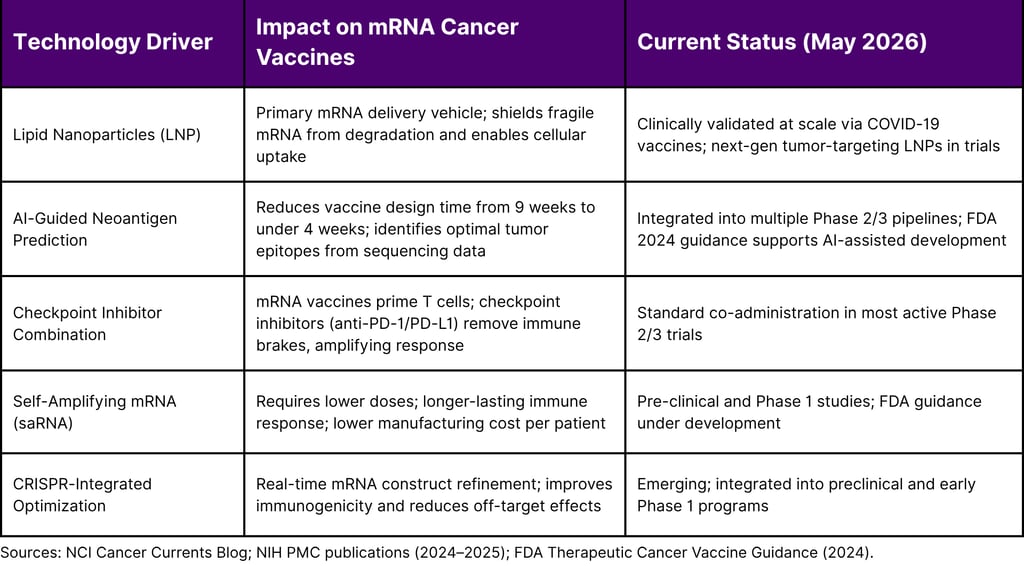
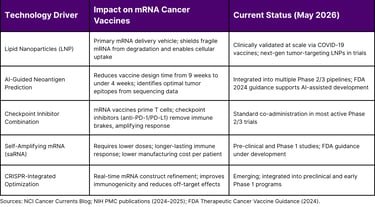
The COVID-19 pandemic accelerated this platform in three decisive ways: it validated lipid nanoparticle (LNP) delivery at massive scale; it attracted billions in public and private capital; and it produced regulatory frameworks that were more agile than before. The NIH, BARDA, and Department of Defense had already laid critical groundwork through investments in mRNA infrastructure. As of 2025, the FDA released comprehensive guidance for therapeutic cancer vaccines, further streamlining the development pathway.
Key Mechanism: How mRNA Cancer Vaccines Work
An mRNA cancer vaccine encodes tumor-specific neoantigens. Once injected, antigen-presenting cells (dendritic cells) translate the mRNA into protein fragments, which are then displayed to cytotoxic T cells. These primed T cells then circulate and eliminate tumor cells bearing the corresponding antigens a highly specific, adaptive immune attack.
The North American mRNA Market: Where We Stand
North America is the undisputed anchor of global mRNA development. The region held approximately 48% of the global mRNA cancer vaccine and therapeutics market share in 2024, driven by the concentration of leading biotechnology firms, the NIH's sustained research funding, and a regulatory environment anchored by the FDA's accelerated pathways. The U.S. government committed approximately $590 million in HHS funding in 2025 to sustain mRNA-related R&D across infectious disease and oncology.
The broader mRNA therapeutics market was valued at approximately $54.84 billion globally in 2024, with North America accounting for the largest regional share. Within the oncology sub-segment where mRNA cancer vaccines reside the market was estimated at $6.25 billion in 2024, with the oncology portion expected to register the highest compound annual growth rate through the next decade, as personalized vaccine pipelines advance from Phase 1/2 to pivotal Phase 3 studies.
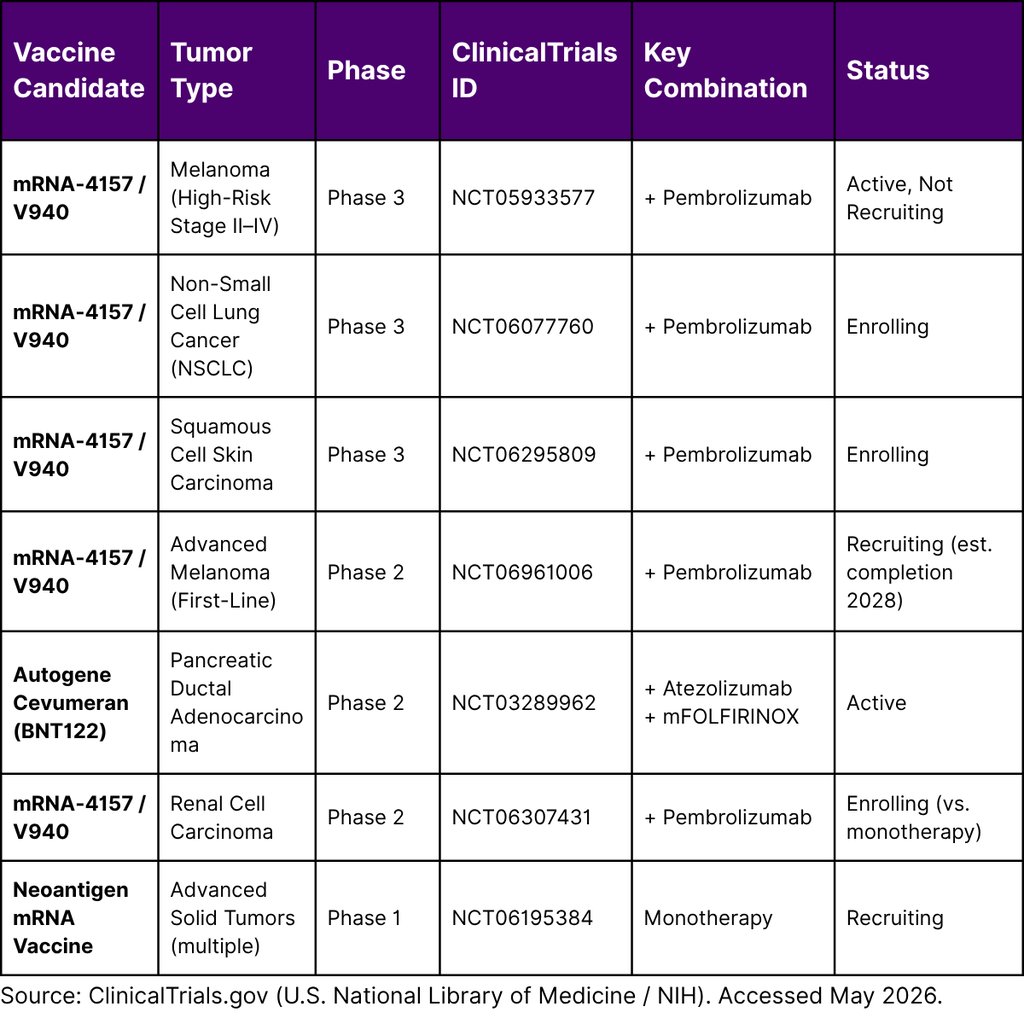
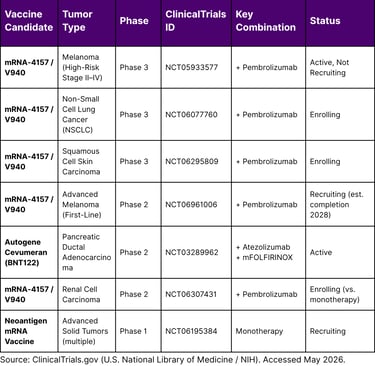
Clinical Trial Landscape: Key mRNA Cancer Vaccine Programs in North America
The ClinicalTrials.gov registry (a U.S. government database maintained by the National Library of Medicine at NIH) provides the most authoritative real-time view of active mRNA cancer vaccine studies. The following table summarizes pivotal programs with North American sites, as of May 2026:
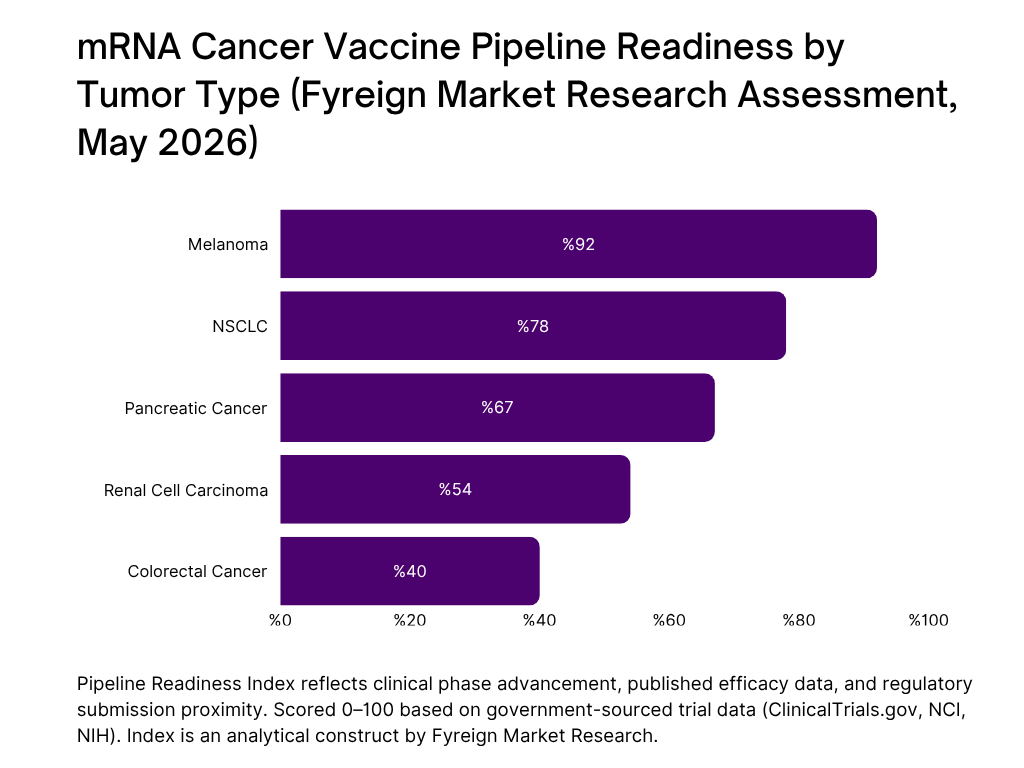
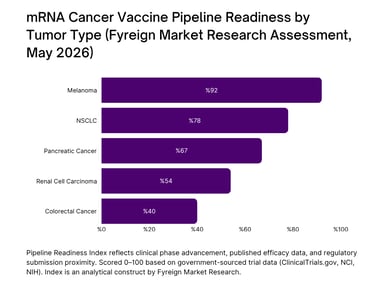
Forecast: Which Solid Tumors Will Integrate First?
Based on clinical trial phase progression, published NIH and NCI data, and the breadth of active regulatory submissions, Fyreign Market Research identifies the following solid tumors as the primary candidates for first successful mRNA vaccine integration in North America:
Melanoma
Highest Likelihood · 2026–2027
Melanoma's high tumor mutational burden and responsiveness to checkpoint inhibitors make it the ideal model for mRNA neoantigen vaccines. The Phase 2b KEYNOTE-942 trial demonstrated a 44% reduction in recurrence risk when mRNA-4157 was added to pembrolizumab. Three-year follow-up data confirmed sustained recurrence-free survival superiority. A Phase 3 program (NCT05933577) is active across multiple countries. Regulatory submission is anticipated in 2026.
ClinicalTrials.gov: NCT05933577 (Phase 3)
01
Non-Small Cell Lung Cancer (NSCLC)
Highest Likelihood · 2027–2028
NSCLC is the most common form of lung cancer and one of the leading causes of cancer mortality in North America. A Phase 3 trial of mRNA-4157 plus pembrolizumab is actively enrolling (NCT06077760), and BioNTech's BNT116 designed to target common NSCLC tumor markers initiated global trials in August 2024. The NSCLC pipeline is expansive; over 50% of patients with NSCLC do not survive beyond 3.5 years post-diagnosis, creating urgent unmet need.
ClinicalTrials.gov: NCT06077760 (Phase 3); BNT116 global trials
02
Pancreatic Ductal Adenocarcinoma
03
Highest Likelihood · 2028–2029
Pancreatic cancer is one of the most lethal malignancies, with a 5-year survival rate under 12%. The personalized mRNA vaccine autogene cevumeran (BNT122) demonstrated vaccine-induced immune responses persisting nearly four years after treatment in some patients, with reduced recurrence risk at 3-year follow-up compared to non-responders. These results, published from Phase 1 data, have propelled Phase 2 expansion and represent one of the most significant oncology breakthroughs of 2024–2025.
NCT03289962; BNT122 Phase 1/2 results (NIH/PMC)
Renal Cell Carcinoma
moderate high · 2028–2030
04
A Phase 2 trial (NCT06307431) is evaluating mRNA-4157 in combination with pembrolizumab in renal cell carcinoma, assessing whether it outperforms checkpoint inhibitor monotherapy. The immunogenicity characteristics of RCC with established responsiveness to immunotherapy make it a logical extension of the mRNA vaccine platform already validated in melanoma.
ClinicalTrials.gov: NCT06307431
Enabling Technologies Accelerating North American Adoption
Market Outlook: North America, 2026–2030
The commercial trajectory of mRNA cancer vaccines in North America is shaped by several converging forces. First, melanoma regulatory submissions anticipated in 2026 could produce the first FDA-approved mRNA cancer vaccine by 2027 a watershed moment that would unlock broad oncology market expansion. Second, NIH and government funding infrastructure, including the approximately $590 million in HHS commitments in 2025, ensures continued clinical trial activity even as the private sector scales investment.
Third, manufacturing improvements have fundamentally altered economics. Production timelines compressed from nine weeks to under four weeks a change that directly impacts the feasibility of personalized vaccine delivery at scale. Cost per patient currently exceeds $100,000, but projections suggest that manufacturing advances and economies of scale may reduce this substantially over the 2026–2030 horizon.
The oncology segment of the mRNA therapeutics market is expected to register the highest growth rate among all application segments through 2030, driven by the expanding personalized medicine pipeline and regulatory momentum. North America's established clinical infrastructure, leadership in AI-driven oncology platforms, and robust NIH grant ecosystem position the region to remain the primary revenue and innovation center for this technology class through the end of the decade.
Frequently Asked Questions
1. Has any mRNA cancer vaccine received FDA approval as of May 2026?
No. As of May 2026, no mRNA cancer vaccine has received full FDA approval for use in cancer treatment, either alone or in combination with other therapies. This is consistent with the NCI's position that while mRNA vaccine technology appears promising for cancer treatment, "these approaches have not yet proven themselves" in a fully regulatory context. The first regulatory submission for a personalized mRNA cancer vaccine (mRNA-4157 / V940 in melanoma) is anticipated in 2026, with potential approval by 2027.
2. What is a neoantigen, and why does it matter for mRNA cancer vaccines?
A neoantigen is a protein fragment produced by a tumor cell as a result of a somatic mutation. Because neoantigens are absent from normal, healthy cells, they are ideal targets for the immune system. mRNA cancer vaccines deliver genetic instructions encoding these neoantigens, prompting the immune system to recognize and attack only cells bearing them improving targeting precision and reducing collateral damage to healthy tissue.
3. Why is melanoma considered the leading candidate for first mRNA cancer vaccine approval?
Melanoma has one of the highest tumor mutational burdens among solid cancers, meaning it produces a large number of neoantigens making it highly visible to an mRNA vaccine-primed immune system. It is also a cancer type with an established history of responding to immunotherapy. The pivotal KEYNOTE-942 Phase 2b trial demonstrated a 44% reduction in recurrence risk with mRNA-4157 plus pembrolizumab, and a Phase 3 trial (NCT05933577) is currently active across multiple countries including North America.
4. How long does it currently take to manufacture a personalized mRNA cancer vaccine?
As of 2025, manufacturing improvements supported by AI-guided neoantigen prediction have reduced the typical production timeline from approximately nine weeks to under four weeks. This represents a significant operational milestone, improving the clinical feasibility of individualized vaccine delivery at scale.
5. What is the current cost of an mRNA cancer vaccine treatment?
mRNA cancer vaccines currently cost over $100,000 per patient a figure consistent across multiple clinical programs. This positions them in the premium-priced personalized medicine segment. Cost-effectiveness analyses suggest justification in adjuvant settings (post-surgery, high relapse risk), where even a modest reduction in recurrence translates to substantial downstream savings. Costs are expected to decrease as manufacturing scales and AI-driven production optimizes efficiency.
6. How many mRNA cancer vaccine trials are currently active globally?
As of 2025, over 120 RNA cancer vaccine trials are active globally, covering malignancies including lung, breast, prostate, melanoma, pancreatic, and brain tumors. The NIH reported approximately 95 personalized neoantigen mRNA vaccine candidates under investigation in 2023, and the pipeline has grown significantly since. North America hosts a substantial share of these trials, anchored by the ClinicalTrials.gov registry maintained by the U.S. National Library of Medicine.
References
National Cancer Institute. (2022, January 20). Can mRNA vaccines help treat cancer? NCI Cancer Currents Blog.
National Institutes of Health / National Library of Medicine – ClinicalTrials.gov. (2025). A Phase 3, Randomized, Double-Blind, Placebo- and Active-Comparator-Controlled Clinical Study of Adjuvant V940 (mRNA-4157) Plus Pembrolizumab Versus Adjuvant Placebo Plus Pembrolizumab in Participants With High-Risk Stage II–IV Melanoma (INTerpath-001). NCT05933577.
National Institutes of Health / National Library of Medicine – ClinicalTrials.gov. (2025). A Phase 2, Randomized, Double-Blind, Placebo- and Active-Comparator-Controlled Clinical Study of V940 (mRNA-4157) Plus Pembrolizumab Versus Placebo Plus Pembrolizumab in Participants With First-Line Advanced Melanoma (INTerpath-012). NCT06961006.
National Institutes of Health / National Library of Medicine – ClinicalTrials.gov. (2024). Anti-cancer Neoantigen mRNA Vaccine to Treat Advanced Solid Tumors: Phase I Clinical Trial. NCT06195384.
National Institutes of Health / National Library of Medicine – ClinicalTrials.gov. (2023). Clinical Study on the Treatment of Advanced Malignant Solid Tumors With the Combination of mRNA Personalized Tumor Vaccine. NCT05949775.
National Institutes of Health / National Library of Medicine – ClinicalTrials.gov. (2017). A Phase 1, Open-Label, Multicenter Study to Assess the Safety, Tolerability, and Immunogenicity of mRNA-4157 Alone and in Combination in Participants With Solid Tumors (KEYNOTE-603). NCT03313778.
Magoola, M., & Niazi, S. K. (2025). Current progress and future perspectives of RNA-based cancer vaccines: A 2025 update. Cancers, 17(11), 1882. (Published on PubMed Central, NIH)
Miao, L., Zhang, Y., & Huang, L. (2021). mRNA vaccine for cancer immunotherapy. Molecular Cancer, 20(1), 1–23. (Published on PubMed Central, NIH)
Ibragimova, A. A., Fedorov, A. A., Kirilenko, K. M., Choynzonov, E. L., Denisov, E. V., & Patysheva, M. R. (2025). mRNA-based personalized cancer vaccines: Opportunities, challenges and outcomes. Acta Naturae. (Published on PubMed Central, NIH)
U.S. Food and Drug Administration. (2024). Guidance for industry: Therapeutic cancer vaccines. U.S. Department of Health and Human Services.
Navigation
© 2026 FyreIgnis Market Research. All rights reserved.
Legal
info@fyreignismarketresearch.com
India
